Shoulder Impingement
Updated:
What is shoulder impingement?
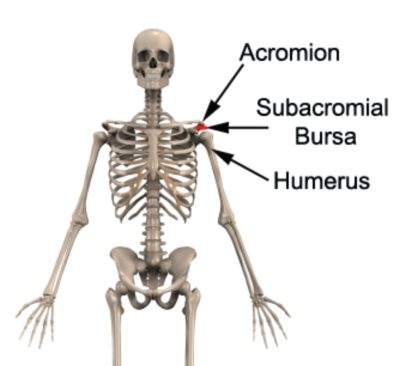
Shoulder impingement is a condition characterized by pinching or compression of soft tissue, such as the rotator cuff tendons and the subacromial bursa, between the upper arm bone (humerus) and roof of the shoulder (acromion) during certain movements of the shoulder, such as arm elevation.
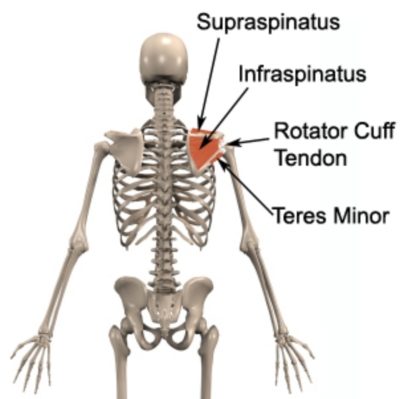
The shoulder joint is a ball and socket joint. The socket arises from the outer aspect of the shoulder blade, whilst the ball arises from the upper aspect of the humerus (upper arm bone). Just above the ball and socket joint of the shoulder is a bony prominence known as the acromion (figure 1). Beneath the acromion lie the tendons of the rotator cuff muscles and the subacromial bursa (figures 1 & 2). The rotator cuff muscles are a group of four muscles (supraspinatus, infraspinatus, subscapularis and teres minor) which primarily act to stabilize the shoulder joint and assist with shoulder movements (figure 2). A bursa is a small sac filled with lubricating fluid, designed to reduce friction between adjacent soft tissue or bony layers. The subacromial bursa reduces friction between the bony prominence of the acromion (above the bursa) and the rotator cuff tendons (in particular the supraspinatus tendon, which attaches to the upper aspect of the humeral head – below the bursa).
Occasionally due to injury associated with overuse or a specific incident, the rotator cuff tendons or subacromial bursa may become damaged, swollen and inflamed. As a result of the swelling, the rotator cuff tendons or subacromial bursa may occupy more space and can subsequently become compressed or pinched during certain movements of the arm, such as elevation (as the humeral head below moves towards the acromion above). Several other postural, biomechanical or anatomical anomalies (such as bony spurs or arthritis) may also contribute to this process. When this occurs the condition is known as shoulder impingement. Shoulder impingement can also sometimes involve the long head of biceps tendon.
Causes of shoulder impingement
Since the rotator cuff tendons and subacromial bursa lie in a very small space between the acromion and humerus, anything that narrows this space may cause shoulder impingement. Shoulder impingement most commonly occurs in association with rotator cuff tendonitis or subacromial bursitis (i.e. inflammation of the tendon(s) or bursa respectively). These conditions typically occur due to repetitive or prolonged activities placing strain on the rotator cuff tendons and/or subacromial bursa. This may occur during repetitive arm elevation activities, overhead activities, reaching activities far away from the body, activities involving rotation of the shoulder, lifting (especially overhead), pushing or pulling activities, placing weight through the affected arm or lying on the affected side. Occasionally, these conditions may occur suddenly due a direct blow to the point of the shoulder, a heavy or awkward lift or due to a fall onto the shoulder, elbow or outstretched hand. Patients with muscle imbalances, shoulder instability, poor posture, or poor shoulder blade control may also have an increased likelihood of developing shoulder impingement.
In athletes, shoulder impingement is commonly seen in throwing sports (such as cricket or baseball), swimming (particularly freestyle and butterfly), racquet sports (such as tennis), weight lifting or paddling sports (such as kayaking). Anomalies to the acromion bone, degenerative changes to the AC joint, or bony spurs known as osteophytes, may also predispose a patient to developing shoulder impingement.
Signs and symptoms of shoulder impingement
Patients with shoulder impingement typically experience pain at the top, front, back or outer aspect of the shoulder. Pain may also radiate into the upper arm as far as the elbow, usually along the outer aspect or down the biceps muscle. Symptoms typically increase during activities that compress the rotator cuff tendons or subacromial bursa. These activities may include arm elevation activities, overhead activities, reaching activities, shoulder rotating activities, lifting, throwing, pushing or pulling, placing weight through the arm or lying on the affected side. In patients with minor shoulder impingement, little or no symptoms may be present. Some patients may experience pain on commencing activity that reduces as they warm up. These patients are usually able to continue sport or activity only to have an increase in pain, ache or stiffness upon resting later (particularly that night or the following morning).
As the condition progresses, patients may experience restricted shoulder range of movement and symptoms that increase during activity or sport, affecting performance. Patients with shoulder impingement may also experience pain on firmly touching the top / outer aspect of the shoulder. A painful arc of arm elevation and / or a feeling of shoulder weakness may also be present particularly when attempting to lift, throw or elevate the arm overhead.
Diagnosis of shoulder impingement
A thorough subjective and objective examination from a physiotherapist is usually sufficient to diagnose shoulder impingement. An ultrasound investigation is commonly used to identify associated conditions, such as rotator cuff tendonitis or subacromial bursitis, and may also demonstrate shoulder impingement on assessment during arm elevation. Further investigations such as an X-ray, CT or MRI scan are often used to assist diagnosis and determine the presence of other conditions.
Prognosis of shoulder impingement
Most patients with this condition heal well with appropriate physiotherapy and return to normal function in a number of weeks. Occasionally, rehabilitation can take significantly longer and may take many months in those who have had their condition for a long period of time, or, in those with other associated significant injuries such as shoulder instability, rotator cuff pathology or degenerative bony changes, such as arthritis. Early physiotherapy treatment is vital to hasten recovery in all patients with shoulder impingement.
Treatment for shoulder impingement
Most cases of shoulder impingement settle well with appropriate physiotherapy. The success rate of treatment for this condition is largely dictated by patient compliance. One of the key components of treatment is that the patient rests from any activity that increases their pain until they are symptom free. Activities which place large amounts of compressive forces through the rotator cuff and subacromial bursa should be minimized, these may include: arm elevation or overhead activities, reaching away from the body, throwing, heavy lifting, pushing or pulling and sleeping or lying on the affected side. Resting from aggravating activities ensures that the body can begin the healing process in the absence of further tissue damage. Once the patient can perform these activities pain free, a gradual return to these activities is indicated provided there is no increase in symptoms.
Ignoring symptoms or adopting a ‘no pain, no gain’ attitude is likely to cause further damage and lead to the condition becoming chronic. Immediate, appropriate treatment in patients with shoulder impingement is essential to ensure a speedy recovery. Once the condition is chronic, healing slows significantly resulting in markedly increased recovery times and an increased likelihood of future recurrence.
Patients with shoulder impingement should follow the R.I.C.E. Regime in the initial phase of injury. The R.I.C.E regime is beneficial in the first 72 hours following injury onset or when inflammatory signs are present (i.e. morning pain or pain with rest). The R.I.C.E. regime for shoulder impingement primarily involves resting from aggravating activities and regular icing. Anti-inflammatory medication may also significantly hasten the healing process by reducing the pain and swelling associated with inflammation.
Manual “hands-on” therapy from the physiotherapist such as massage, trigger point releases, joint mobilisation, manipulation, dry needling, stretches and electrotherapy can also assist with hastening healing and improving flexibility and function in patients with this condition.
Patients should also undergo a graduated flexibility and strengthening program of the surrounding muscles to ensure an optimal outcome. Particular emphasis is placed on improving shoulder blade stability, posture and rotator cuff function. The treating physiotherapist can advise which exercises are most appropriate for the patient and when they should be commenced.
Often, a corticosteroid injection by a sports physician into the subacromial bursa or affected rotator cuff tendon is effective in reducing symptoms and allowing earlier rehabilitation progression.
In the final stages of rehabilitation, a gradual return to activity or sport can occur as guided by the treating physiotherapist provided there is no increase in symptoms.
In patients with significant pathology involving major rotator cuff pathology and/or bony spurring, orthopaedic surgery may be considered to improve the condition.
Contributing factors to the development of shoulder impingement
There are several factors which can predispose patients to developing shoulder impingement. These need to be assessed and corrected with direction from a physiotherapist. Some of these factors include:
- joint stiffness (particularly the shoulder, neck or upper back)
- shoulder instability
- bony anomalies of the acromion or AC joint
- muscle tightness (particularly the rotator cuff, pectorals and deltoid)
- poor posture
- inappropriate or excessive training
- inadequate warm up
- muscle weakness (especially the rotator cuff and scapula stabilisers)
- muscle imbalances
- inadequate rehabilitation following a previous shoulder injury or surgery
- inappropriate technique (e.g. swimming stroke, tennis serve, throwing technique)
Physiotherapy for shoulder impingement
Physiotherapy treatment is vital to hasten the healing process, ensure an optimal outcome and reduce the likelihood of recurrence in all patients with shoulder impingement. Treatment may comprise:
- soft tissue massage
- electrotherapy (e.g. ultrasound, TENS etc)
- stretches
- joint mobilization
- joint manipulation
- ice or heat treatment
- exercises to improve strength, flexibility, posture and scapula stability
- correction of abnormal biomechanics or technique
- education
- postural taping
- the use of a posture support
- anti-inflammatory advice
- activity modification advice
- a gradual return to activity program
Other intervention for shoulder impingement
Despite appropriate physiotherapy management, some patients with this condition do not improve adequately. When this occurs the treating physiotherapist or doctor will advise on the best course of management. This may include further investigations such as X-rays, ultrasound, MRI or CT scan, pharmaceutical intervention, corticosteroid injection or referral to appropriate medical authorities who will advise on any interventions that may be appropriate to improve the condition. In severe cases that are unresponsive to conservative measures, surgical intervention may be indicated.
Exercises for shoulder impingement
The following exercises are commonly prescribed to patients with shoulder impingement. You should discuss the suitability of these exercises with your physiotherapist prior to commencing them. Generally, they should be performed 1 – 3 times daily and only provided they do not cause or increase symptoms.
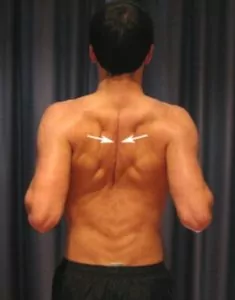
Shoulder Blade Squeezes
Begin sitting or standing tall with your back straight (figure 3). Squeeze your shoulder blades together as far as possible pain free. Hold for 5 seconds and repeat 10 times provided there is no increase in symptoms.
Pendular Exercises
Begin this exercise by leaning forwards with your good forearm supported on a table or bench (figure 4). Keeping your back straight and your shoulder relaxed, gently swing your affected arm forwards and backwards as far as possible pain free. Repeat the exercise swinging your arm side to side as far as possible pain free. Repeat 10 times in each direction provided there is no increase in symptoms.

Pendular Circles
Begin this exercise by leaning forwards with your good forearm supported on a table or bench (figure 5). Keeping your back straight and your shoulder relaxed, gently swing your affected arm in circles clockwise as far as possible pain-free. Repeat the exercise swinging your arm counter clockwise. Repeat 10 times in each direction provided there is no increase in symptoms.

Physiotherapy products for shoulder impingement
Some of the most commonly recommended products by physiotherapists to hasten healing and speed recovery in patients with shoulder impingement include:






To purchase physiotherapy products for shoulder impingement click on one of the above links or visit the PhysioAdvisor Shop.
Find a Physio for shoulder impingement
Find a physiotherapist in your local area who can treat shoulder impingement.
More Information
- View more Shoulder Stretches.
- View Shoulder Strengthening Exercises.
- View Rotator Cuff Strengthening Exercises.
- View Postural Taping.

Link to this Page
If you would like to link to this article on your website, simply copy the code below and add it to your page:
<a href="https://physioadvisor.com.au/injuries/shoulder/shoulder-impingement”>Shoulder Impingement – PhysioAdvisor.com</a><br/>PhysioAdvisor provides detailed physiotherapy information on shoulder impingement including: causes, symptoms, diagnosis, treatment, exercises, physiotherapy products and more...
Return to the top of Shoulder Impingement.